Endometriosis tissue acts as the lining inside the uterus would - it thickens, breaks down and bleeds with each menstrual cycle. But it grows in places where it doesn't belong, and it doesn't leave the body. When endometriosis involves the ovaries, cysts called endometriomas may form. Surrounding tissue can become irritated and form scar tissue. Bands of fibrous tissue called adhesions also may form. These can cause pelvic tissues and organs to stick to each other.Other form is the adenomyosis, in which the uterus muscular layer is thickened because of endometriosis cell within the myometrium.

ENDOMETRIOSIS
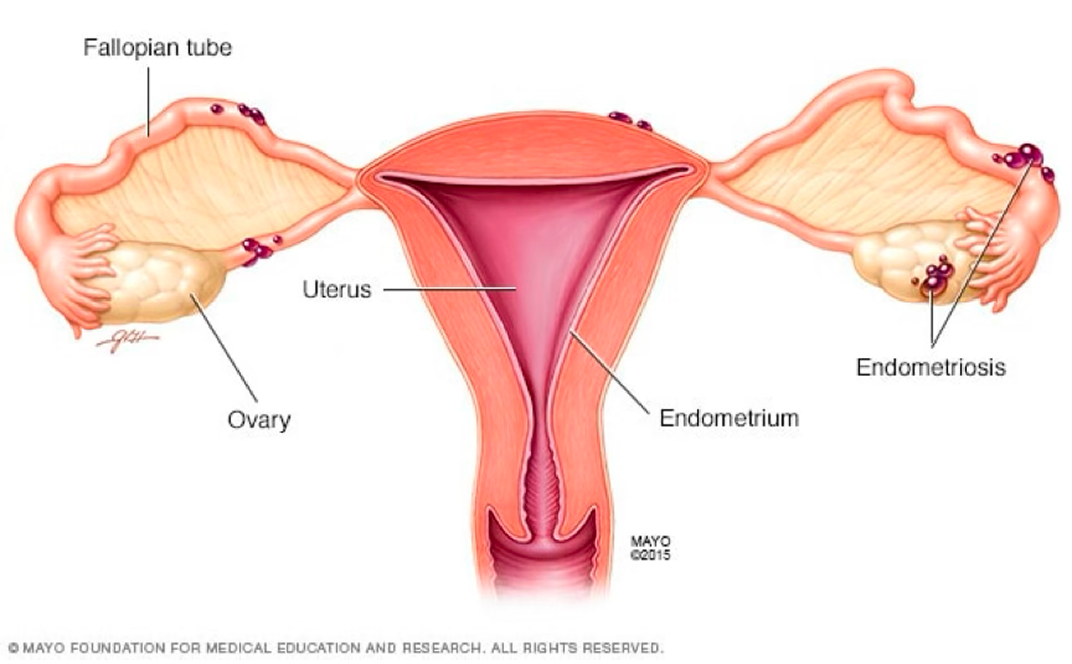
Endometriosis is a disease condition in which tissue that is similar to the inner lining of the uterus grows outside the uterus. It often affects the ovaries, fallopian tubes and the tissue lining the pelvis, on the outside surface of the uterus, or the tissues surrounding the uterus and the ovaries. Rarely, endometriosis growths may be found beyond the area where pelvic organs are located.
Symptoms
The main symptom of endometriosis is pelvic pain. Symptoms vary widely between individuals. Some have no symptoms, while for others it can be a debilitating disease. It's often linked with menstrual periods. Although many people have cramping during their periods, those with endometriosis often describe menstrual pain that's far worse than usual. The pain also may become worse over time.
Common symptoms of endometriosis include:
- Menstrual pain. Pelvic pain and cramping may start before a menstrual period and last for days into it. You also may have lower back and stomach pain. Another name for painful periods is dysmenorrhea.
- Heavy menses. Sometimes, you may have heavy menstrual periods or bleeding between periods.
- Pelvic pain. Uncomfortable lower abdomen / back pain during or outside the menstrual period.
- Infertility. For some people, endometriosis is first found during tests for infertility treatment.
- Pain with sex. Pain during or after sex is common with endometriosis.
- Pain with bowel movements or urination. You're most likely to have these symptoms before or during a menstrual period.
A presumed diagnosis can be made based on symptoms and medical imaging; a laparoscopy (keyhole surgery) with a biopsy can provide definite confirmation. Other causes of similar symptoms include adenomyosis, uterine fibroids, irritable bowel syndrome, and interstitial cystitis.
While there is no cure for endometriosis, several treatments may improve symptoms. This includes pain medication, hormonal treatments or surgery. The recommended pain medication is usually a non-steroidal anti-inflammatory drug (NSAID), such as mefenamic acid or naproxen. Taking the birth control pill continuously or using a hormonal coil (coil) is another first-line treatment. Other types of hormonal treatment can be tried if the pill or IUD are not effective. Endometriosis can be removed surgically in women whose symptoms are not relieved by other treatments or to help with infertility.
Surgery
Laparoscopy the uterus and fallopian tubes. The abdomen is filled with gas so that the surgeon can see better and have space for instruments.
Clinical guidelines recommend surgery when medical treatment does not work sufficiently, has unacceptable side effects or is contraindicated. Large endometriomas can only effectively be treated with surgery. Surgery is also recommended when deep endometriosis causes problems in the bowels or bladder, such as obstruction. It is unclear what the effect of surgery is for pain relief in cases of superficial peritoneal endometriosis.
Laparoscopy (keyhole surgery) is the standard surgical approach. Treatment consists of the removal of endometriosis and the restoration of pelvic anatomy via the division of adhesions.
With laparoscopic surgery, small instruments are inserted through incisions to remove the endometriosis tissue and adhesions. After surgery, people can usually return home the same day.
Endometriomas are usually excised (removed completely). Compared to drainage and coagulation of the cyst, excision makes it less likely the cysts and pain symptoms come back. For deep endometriosis, surgery improves quality of life and pain symptoms. However, the procedure can be complicated, especially if the lesions are in or near the bowel, ureter of the urinary system or the chest, and requires a interdisciplinary surgical team in those cases. For instance, for rectovaginal endometriosis, 7% of surgeries had complications. Sometimes, a part of the bowel or bladder is removed. For women who still have significant pain after hormonal treatment and other surgery, and do not want to become pregnant, a hysterectomy (removal of the womb) can be offered. This is done in combination with removal of endometriosis lesions. Removal of the womb may be beneficial if the uterus itself is affected by adenomyosis.
When to see a doctor
See a member of your health care team if you think you might have symptoms of endometriosis.
Endometriosis can be a challenge to manage. You may be better able to take charge of the symptoms if:
- Your care team finds the disease sooner rather than later.
- You learn as much as you can about endometriosis.
- You get treatment from a team of health care professionals from different medical fields if needed.